How do tumors metastasize and spread? In most cancers, this happens through a metastasis cascade during which cancer cells progressively acquire the ability to invade, survive in circulation, colonize distant organs, and build a network for growth. Together, invasion and metastasis account for the majority of cancer-related deaths from solid tumors and represent a defining hallmark of malignant cancer progression.
This blog covers the metastatic cascade from early events in the primary tumor to local invasion, intravasation to blood vessels, circulation throughout the body, and extravasation and colonization of distant organs, highlighting key molecular events that enable this cancer hallmark and how it is being targeted therapeutically.
< Jump to the product list at the end of this blog >
Early Changes in the Tumor Microenvironment
|
At the primary tumor site, cancer cells, cancer-associated fibroblasts (CAFs), endothelial cells, and other tumor‑associated stromal and immune cells work together to create a tumor microenvironment (TME) that enables invasion and metastasis. Hypoxia is a central driver of this process—the activation of hypoxia‑inducible factor (HIF) signaling upregulates hundreds of genes involved in angiogenesis, metabolism, chronic inflammation, and extracellular matrix (ECM) remodeling, helping to prime the tumor for malignant behavior. |
 Activating Invasion and Metastasis is one of the original six cancer hallmarks, first described in 2000.
Activating Invasion and Metastasis is one of the original six cancer hallmarks, first described in 2000.These changes lead to elevated levels of factors such as IL‑1, PDGF, TGF‑β, IL‑6, and the activation of CAFs, which are often characterized by markers including α‑smooth muscle actin, fibroblast‑specific protein (FSP), and fibroblast activation protein (FAP). Together, these signals remodel the ECM, increase tissue stiffness, and give tumor cells a survival and motility advantage that facilitates the first steps of the metastasis cascade by promoting local invasion into surrounding tissue.
 |
 |
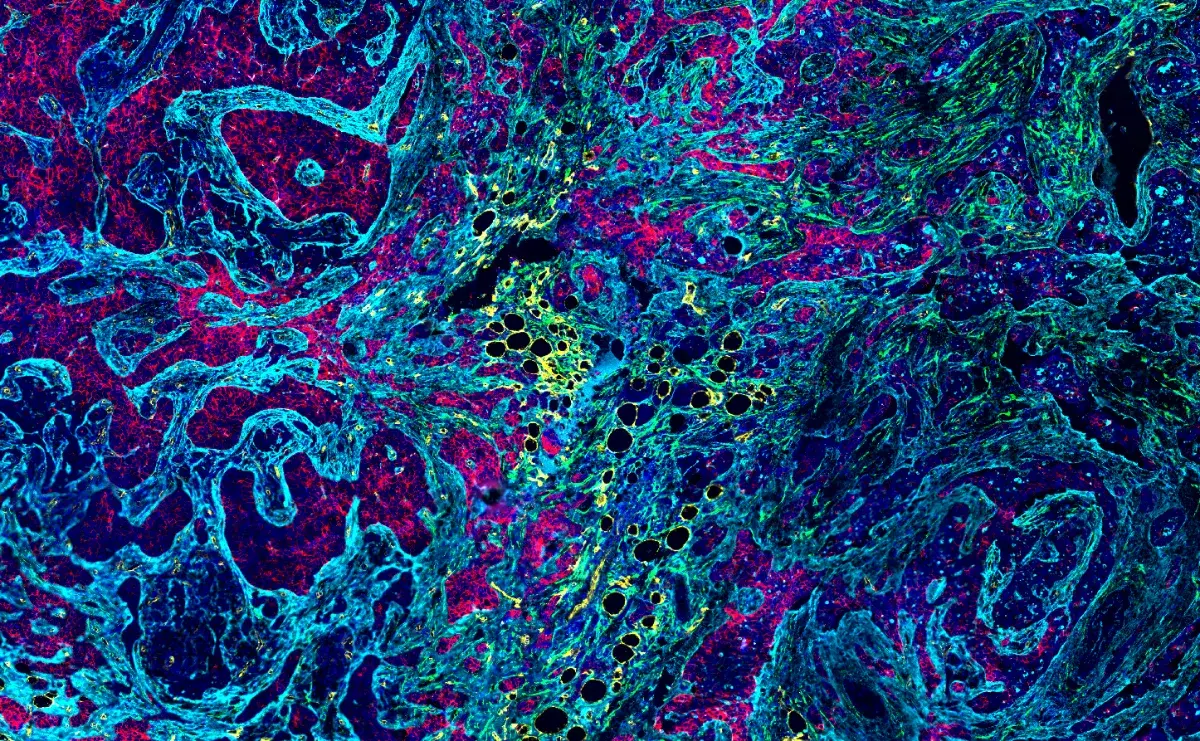
| Immunohistochemical (IHC) analysis of paraffin-embedded human gastrointestinal stromal tumor using HIF-1α (E1V6A) Rabbit Monoclonal Antibody #48085 performed on the BOND RX Fully Automated Research Stainer by Leica Biosystems. | IHC analysis of paraffin-embedded human endometrioid carcinoma using alpha-Smooth Muscle Actin (D4K9N) Rabbit Monoclonal Antibody #19245 performed on the Leica Bond RX. |
Relevant Pathway
 |
Hypoxia SignalingUnder low-oxygen conditions, hypoxia-inducible factors (HIFs) detect hypoxia and reprogram gene expression to regulate angiogenesis, metabolism, extracellular matrix remodeling, and immune responses. Download the Hypoxia Signaling pathway diagram |
Epithelial–Mesenchymal Transition
Epithelial–mesenchymal transition (EMT) is an important step in tumor progression during which epithelial cancer cells lose their adhesion and acquire motility. During EMT, transcription factors such as SNAIL, ZEB, and TWIST repress epithelial genes (e.g., E‑cadherin) and upregulate mesenchymal markers (e.g., N‑cadherin and vimentin), leading to loss of polarity, weakened cell-cell junctions, and a spindle‑like morphology.
Simultaneously, HIF-α and TGF‑β‑activated primary tumor cells and associated CAFs secrete matrix metalloproteinases (MMPs), lysyl oxidase (LOX) family enzymes, and collagens that help degrade and reorganize the local ECM. MMPs help cancer cells breach basement membranes, while LOX‑mediated collagen crosslinking stiffens the ECM and lays down collagen fiber “tracks” that guide migrating tumor cells toward intravasation sites for dissemination.
 |
 |
| IHC analysis of paraffin-embedded human breast carcinoma using MMP-9 (D6O3H) Rabbit Monoclonal Antibody #13667. |
IHC analysis of paraffin-embedded human endometrioid adenocarcinoma using COL1A1 (E8F4L) Rabbit Monoclonal Antibody #72026 performed on the Leica BOND RX. |
Relevant Pathways





Invadopodia Formation, Intravasation, and Angiogenesis
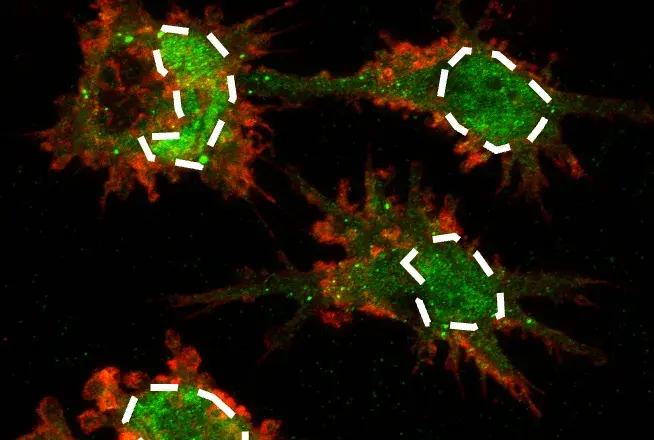
To degrade the ECM and enable entry into the bloodstream or lymphatic vessels, invasive tumor cells assemble invadopodia—actin‑rich protrusions that focus proteolytic enzyme activity at the invasion front. Invadopodia formation is stimulated by growth factors and cytokines secreted by tumor cells and CAFs, including VEGF and FGF, and is characterized by the presence of cortactin, TKS5, and membrane‑tethered MMP14 (MT1‑MMP) at the invasion front.
 |
 |
| IHC analysis of paraffin-embedded human prostate adenocarcinoma using Basic FGF (E5Y6M) Rabbit Monoclonal Antibody #46879 highlights FGF expression by tumor cells. |
Western blot analysis of extracts from various cell lines using VEGF-A (E9X8Q) Rabbit Monoclonal Antibody #50661 (upper) or GAPDH (D16H11) Rabbit Monoclonal Antibody #5174 (lower). Negative expression of VEGF-A protein in HuT 102 cells is consistent with the predicted expression pattern. |
At the same time, tumor- and CAF-derived VEGF and FGF initiate angiogenesis, which not only drives the formation of abnormal, leaky tumor vasculature to create sites for intravasation, but also forms the new blood vessels that supply nutrients to malignant tumor sites known as tumor angiogenesis.
Relevant Pathway
 |
Tumor AngiogensisSee how angiogenic signals regulate the growth and remodeling of blood vessels, including how factors such as VEGF, FGF, PDGF, angiopoietins, integrins, and MMPs coordinate endothelial sprouting, migration, and vessel maturation under hypoxic conditions. Get the Tumor angiogenesis pathway diagram |
Immune Evasion During Dissemination
As tumor cells enter and travel through the bloodstream, they remain closely linked to an immunosuppressive microenvironment that helps them evade immune detection and clearance. Tumor cells and CAFs secrete factors such as CSF (G‑CSF), MCP‑1 (CCL2), IL‑6, IL‑1β, and CXCL12 (SDF1) to recruit myeloid‑derived suppressor cells (MDSCs) and tumor‑promoting M2 macrophages, often marked by CD163 and CD206.
MDSCs and M2 macrophages release immunosuppressive mediators, including Arginase‑1, IL‑10, and PD‑L1, which dampen cytotoxic T cell responses and protect associated tumor aggregates during intravasation and circulation. This immunosuppressive population functions as a mobile shield that accompanies clusters of circulating tumor cells, increasing their chances of surviving immune attack in the bloodstream.
 |
 |
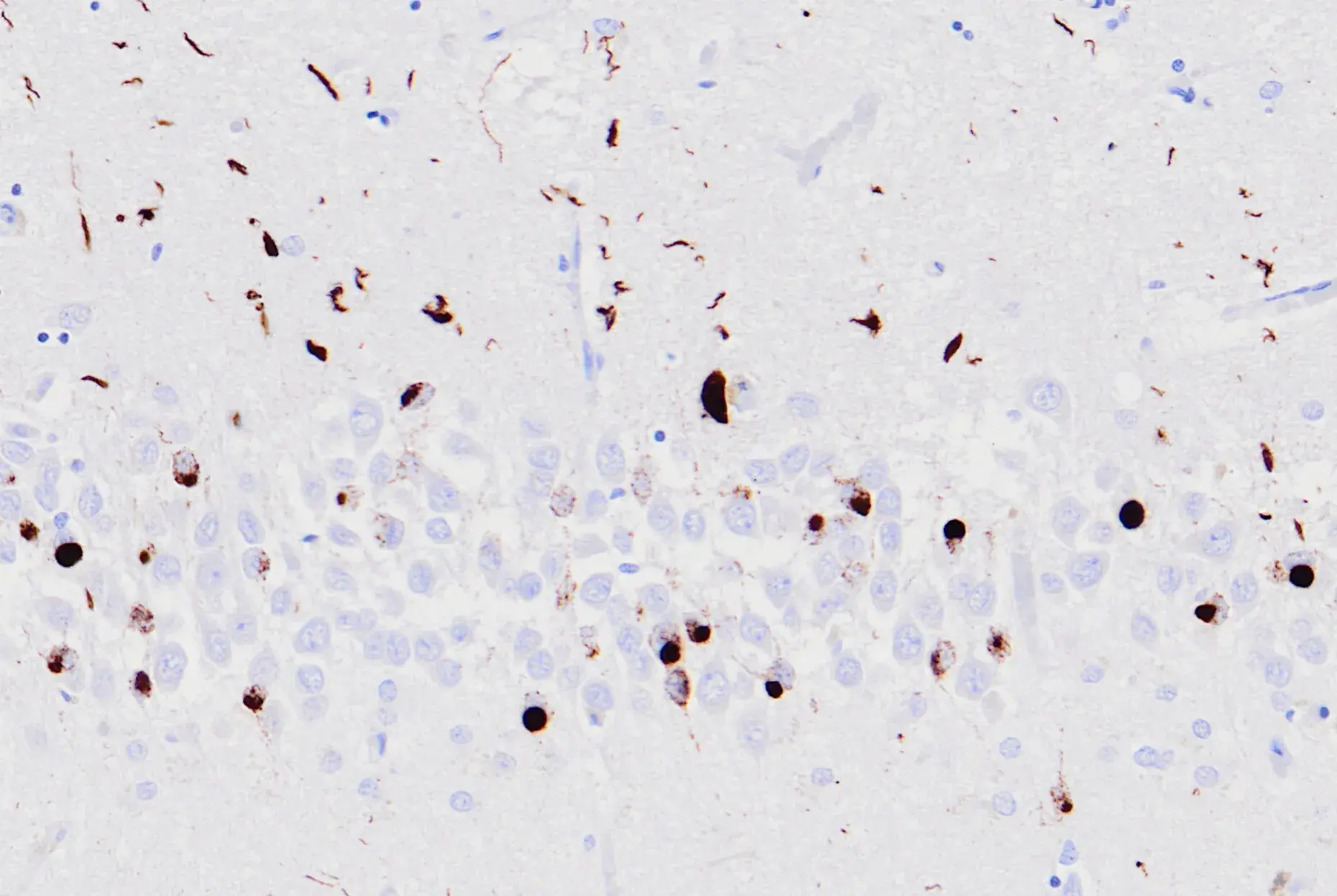
| IHC analysis of paraffin-embedded human colon adenocarcinoma using Arginase-1 (D4E3M™) Rabbit Monoclonal Antibody #93668 performed on the Leica BOND RX. | IHC analysis of paraffin-embedded human non-small cell lung carcinoma using PD-L1 (E1L3N®) Rabbit Monoclonal Antibody #13684 performed on the Leica BOND RX. |
Relevant Pathway

Blog: What are myeloid cells and how are they identified?
Extravasation and Vascular “Hot Spots”
Successful metastasis to a new organ also requires tumor cells to exit the vasculature at specific “hot spots” of extravasation, where local endothelial activation and junction remodeling create sites for tumor escape into the surrounding tissue. These hot spots can be initiated both by local inflammatory cytokines and by tumor‑derived factors and extracellular vesicles that are delivered to distant organs, where they activate endothelial cells, increase vascular permeability, and help pre‑establish a permissive premetastatic niche. At these sites, tumor and monocyte-derived cytokines and chemokines promote endothelial activation and retraction, partly via E‑selectin upregulation, enabling transient adhesion of circulating tumor cells to the vessel wall.
Following this, stable adhesion is established through interactions between tumor cell integrins and adhesion molecules such as ICAM-1 (CD54) and ALCAM on endothelial cells, together with endothelial receptors including ICAM-1, VCAM-1, and lamin-rich basement membrane components that anchor adherent tumor cells to the vessel wall. Next, tumor-derived VEGF-A activates VEGFR signaling in endothelial cells. Downstream, FAK/Src signaling promotes VE‑cadherin phosphorylation and causes dissociation between VE‑cadherin and β‑catenin complexes at adherens junctions, leading to junction destabilization and opening paracellular routes for tumor extravasation.
 |
 |
| IHC analysis of paraffin-embedded human urothelial carcinoma using CD54/ICAM-1 (E3Q9N) Rabbit Monoclonal Antibody #67836 performed on the Leica BOND RX. | IHC analysis of paraffin-embedded CT26.WT syngeneic tumor using VE-Cadherin (F4K3Y) Rabbit Monoclonal Antibody #60787. |
Together with local stromal and immune cells, these extravasation hot spots act as vascular exit points that disseminated tumor cells exploit to leave the circulation and begin colonizing distant tissues.
Relevant Pathway

Building the Premetastatic Niche
Even before disseminated tumor cells arrive, many primary tumors condition distant organs to form a premetastatic niche (PMN) that favors metastasis. This is accomplished through the secretion of tumor‑type–specific factors and hypoxia‑induced, tumor‑derived extracellular vesicles that travel through the circulation and are selectively taken up by endothelial and stromal cells in select distant organs based on the nature of the primary tumor, where they activate endothelium, increase vascular permeability, and remodel the local ECM to seed a premetastatic niche.
The resulting premetastatic niche (PMN) is rich in cytokines, growth factors, and ECM regulators, including MCP‑1 (CCL2), CXCL12 (SDF1), TGF‑β, TNF, VEGF, LOX, and fibronectin. These function to enhance vascular permeability, stimulate angiogenesis, and recruit immunosuppressive cells—such as MDSCs, macrophages, and regulatory T cells (Tregs)—to ensure tumor survival and growth.
 |
 |
| IHC analysis of paraffin-embedded human ovarian carcinoma using SDF1/CXCL12 (D8G6H) Rabbit Monoclonal Antibody #97958. |
IHC analysis of paraffin-embedded human neuroendocrine carcinoma of the lung using Fibronectin/FN1 (E5H6X) Rabbit Monoclonal Antibody #26836 performed on the Leica BOND RX. |
Therapeutic Interventions Targeting the Metastatic Cascade
Given that invasion and metastasis account for the majority of cancer‑related deaths from solid tumors, multiple therapeutic strategies aim to disrupt distinct steps of the metastasis cascade, including the following:
- Preventing CAF Activation: Inhibition of the Hedgehog signaling pathway using small molecule inhibitors, antibody-based neutralization or inhibition of TGF‑β, and small molecule inhibition of the TGF‑β receptor can reduce CAF activation and dampen pro‑invasive remodeling of the TME.
- Blocking EMT: Antibody-based neutralization or inhibition of TGF‑β, small molecule inhibition of the TGF‑β receptor, and the development of tyrosine kinase inhibitors targeting EGFR aim to prevent or reverse EMT and limit tumor cell motility.
- Interfering with Vascular Remodeling: LOX and LOXL2 inhibition, antibody-based blockade of fibronectin (FN1, including EDA-containing isoforms) function, small molecule inhibition of collagen I (COL1A1) synthesis or crosslinking, and targeting hyaluronan or integrin αV seek to disrupt ECM stiffening, alignment, and cell–matrix signaling that support invasion.
- Targeting Angiogenesis: Antibody-based blockade of the VEGF–VEGFR2 interaction and small molecule inhibition of FGF–FGFR signaling can normalize or regress tumor vasculature and reduce opportunities for intravasation and metastatic growth.
- Targeting Immunosuppressive Factors: Antibody-based blockade of PD‑1, PD‑L1, and CTLA‑4 relieves T cell inhibition and can counteract the immunosuppressive retinue created by MDSCs and M2 macrophages in primary and metastatic sites.
- Suppressing the PMN: LOX and LOXL2 inhibition, CXCL12–CXCR4 blockade with CXCR4 antagonists, small molecule inhibition or antibody blockade of MET, and small molecule targeting of S100A9 aim to prevent or dismantle premetastatic niches before they can be colonized.
Beyond these strategies, researchers are investigating the possibility of targeting additional ECM components by inhibiting tissue-specific collagen I, fibronectin, periostin, and integrins, with the goal of destabilizing both pre‑metastatic and metastatic niches and limiting metastatic growth. Combination therapies are also being explored, such as pairing whole-brain radiation with EGFR tyrosine kinase inhibitors to reduce lung-to-brain metastasis, or combining HER2-targeted inhibitors with the cytotoxic agent capecitabine to limit breast-to-brain spread.
Other potential treatment options include the use of nanoparticles to mediate target-specific drug delivery, such as ultrasmall copper nanoparticles (CuCuOx) targeted to chemokine receptors like CCR2 as nanocarriers loaded with chemotherapeutics such as gemcitabine. Early detection and targeting of PMNs—through direct labeling of upregulated components at the PMN site with specific antibodies or small molecules directed against proteins such as LOX, S100A8/S100A9, or fibronectin—offer additional opportunities to intercept metastasis before overt secondary tumors develop.
As new tools for high‑resolution tumor profiling continue to sharpen our view of the metastasis cascade, they will help uncover additional, druggable vulnerabilities in both tumor cells and their niches. For researchers, integrating these technologies with pathway‑focused reagents offers a powerful way to move from describing invasion and metastasis to actively intercepting them.
Additional Resources
Read the additional blogs in the Hallmarks of Cancer Series:
- Evading Growth Suppressors
- Nonmutational Epigenetic Reprogramming
- Avoiding Immune Destruction
- Tumor-Promoting Inflammation
- Inducing or Accessing Vasculature (Angiogenesis)
- Senescent Cells
- Genome Instability & Mutation
- Resisting Cell Death
- Deregulating Cellular Metabolism
- Unlocking Phenotypic Plasticity
- Sustaining Proliferative Signaling
Select References
- Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100(1):57-70. doi:10.1016/s0092-8674(00)81683-9
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646-674. doi:10.1016/j.cell.2011.02.013
- Hanahan D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022;12(1):31-46. doi:10.1158/2159-8290.CD-21-1059
- Chouaib S, Noman MZ, Kosmatopoulos K, Curran MA. Hypoxic stress: obstacles and opportunities for innovative immunotherapy of cancer. Oncogene. 2017;36(4):439-445. doi:10.1038/onc.2016.225
- Sahai E, Astsaturov I, Cukierman E, et al. A framework for advancing our understanding of cancer-associated fibroblasts. Nat Rev Cancer. 2020;20(3):174-186. doi:10.1038/s41568-019-0238-1
- Lee JJ, Ng KY, Bakhtiar A. Extracellular matrix: unlocking new avenues in cancer treatment. Biomark Res. 2025;13(1):78. Published 2025 May 27. doi:10.1186/s40364-025-00757-3
- Hu D, Li Z, Zheng B, et al. Cancer-associated fibroblasts in breast cancer: Challenges and opportunities. Cancer Commun (Lond). 2022;42(5):401-434. doi:10.1002/cac2.12291
- Gerashchenko TS, Novikov NM, Krakhmal NV, et al. Markers of Cancer Cell Invasion: Are They Good Enough?. J Clin Med. 2019;8(8):1092. Published 2019 Jul 24. doi:10.3390/jcm8081092
- Dupas A, Goetz JG, Osmani N. Extravasation of immune and tumor cells from an endothelial perspective. J Cell Sci. 2024;137(21):jcs262066. doi:10.1242/jcs.262066
- Peinado H, Zhang H, Matei IR, et al. Pre-metastatic niches: organ-specific homes for metastases. Nat Rev Cancer. 2017;17(5):302-317. doi:10.1038/nrc.2017.6
- Li Y, Liu F, Cai Q, et al. Invasion and metastasis in cancer: molecular insights and therapeutic targets. Signal Transduct Target Ther. 2025;10(1):57. Published 2025 Feb 21. doi:10.1038/s41392-025-02148-4