Each year, approximately 13% of all women in the US and 25% of all women globally will feel their hearts drop when they get the news that they have breast cancer.1 It is the most commonly diagnosed cancer, with an estimated 684,996 deaths worldwide in 2020. For the last four decades, October has been recognized as National Breast Cancer Awareness Month, created to raise awareness and bring this number down. This includes educating people about the importance of early detection because the five-year relative survival rate when the cancer is still localized is 99%.2 This becomes especially important for those who inherit a loss of function BReast CAncer (BRCA) mutation, as 55-65% percent of women with the BRCA1 mutation and 45% of women with the BRCA2 mutation will develop breast cancer before the age of 70.2
When someone learns they have a BRCA gene mutation when they are cancer-free, it can influence how early and how diligently their doctors schedule mammograms, and may lead them to consider whether a preventative mastectomy is the right path forward. However, many only learn they carry the BRCA mutation after they are diagnosed. Having the BRCA mutation also influences how one can fight the disease. PARP inhibitors like olaparib are extremely effective when treating BRCA-associated cancers and are the only targeted therapy available for patients who have this mutation. However, recurrence rates, even with PARP inhibitor treatment, is still high. Thus, developing new BRCA-specific therapeutics is sorely needed to realize a future without breast cancer.
BRCA1 and BRCA2—What's the difference?
BRCA1 and BRCA2 mutations both play a role in repairing double-strand DNA breaks and are often not differentiated when referring to types of breast cancer in general literature. However, the difference between these two mutations can be vitally important. Women with the BRCA1 mutation have a slightly higher risk of developing breast cancer compared to women with the BRCA2 mutation. Men with a BRCA1 mutation have a 1-5% lifetime risk of developing male breast cancer, but a 5-10% lifetime risk if the mutation is located in the BRCA2 gene.3 Additionally, cancers with a BRCA1 mutation are more likely to be triple negative, meaning they don't express estrogen receptors, progesterone receptors, or HER2, making them more aggressive and harder to treat. On the other hand, cancers with a BRCA2 mutation are often estrogen receptor-positive.
%20CANCER/23-can-91951/CST50799_IHC_breast%20cancer_BRCA1%20antibody.webp?width=600&height=373&name=CST50799_IHC_breast%20cancer_BRCA1%20antibody.webp)
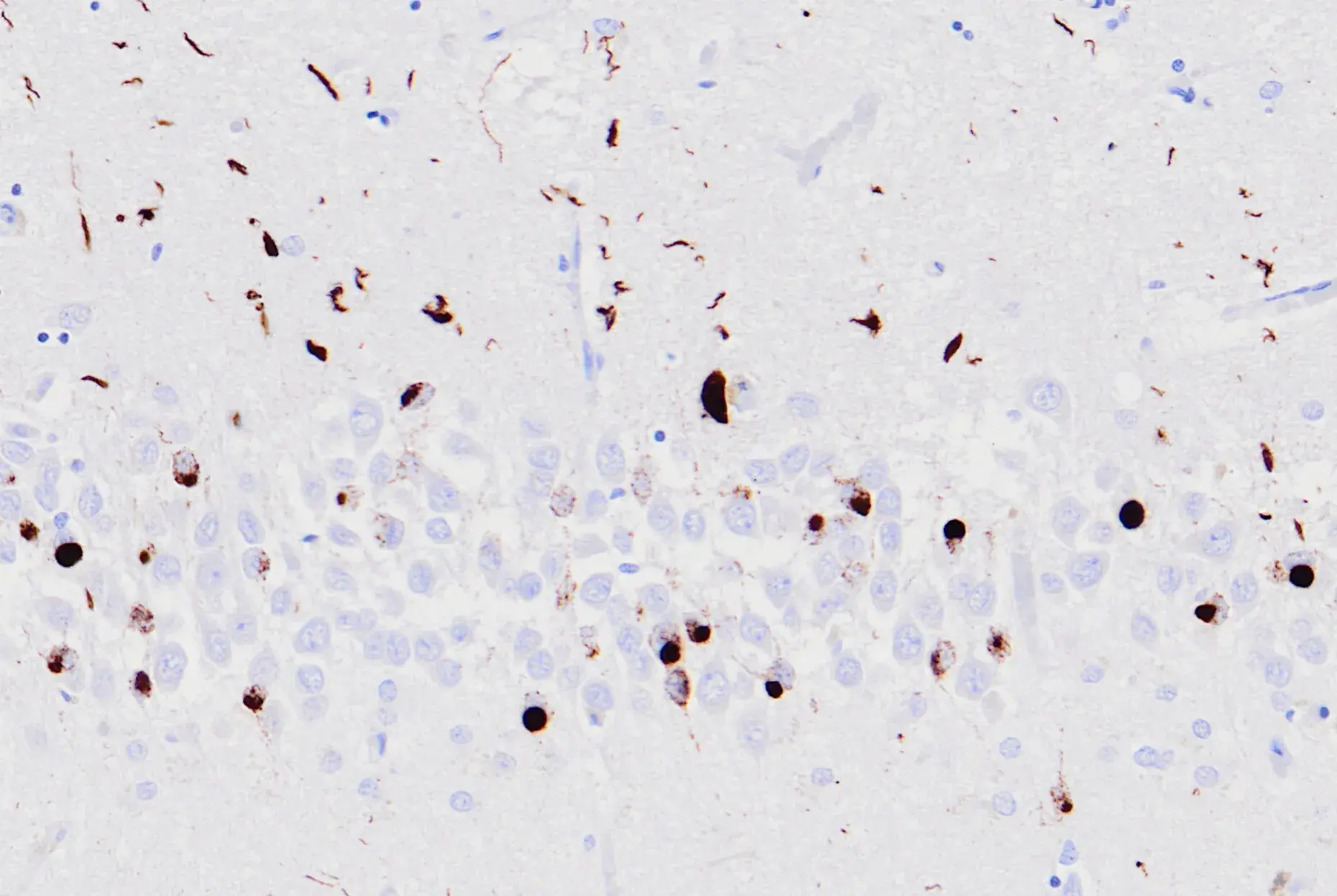
Immunohistochemical analysis of paraffin-embedded human ductal breast carcinoma using BRCA1 (E5S9G) Rabbit mAb #50799 performed on the Leica Bond RX.
Therefore, approaching the two mutations separately may result in more efficacious therapies. Both function in the DNA repair pathway but play different roles.4 BRCA1 is a damage checkpoint activator and repairs DNA, while BRCA2 is a pivotal component required for homologous recombination. Thus, understanding how each gene contributes to tumor initiation and progression could lead to more effective isoform-specific therapies.
 |
Explore the interactive DNA Damage Response Signaling Pathway, along with associated CST antibody products. |
New Therapeutic Approaches to Combat Cancers with the BRCA Mutation
While BRCA1- or BRCA2-specific therapies are still on the horizon, PARP inhibitors are currently the only targeted therapy approved by the FDA for BRCA-related breast cancers. PARP enzymes are involved in DNA repair in response to stress. When they are inhibited, the collective lack of tumor DNA repair due to the loss of PARP- and BRCA-related repair mechanisms leads to cell death.
However, PARP inhibitors as a monotherapy have had limited success in treating breast cancers with the BRCA mutation due to the high percentage of tumors that become resistant. Studies indicate PARP inhibitor resistance can occur due to molecular signaling events that lead to the restoration of homologous recombination, reverse mutations, increased drug efflux, and restoration of the replication fork.5 Additional analysis of matched primary and recurrent tumors with BRCA1 or BRCA2 mutations has yielded isoform-specific insights into how the tumors can become resistant.6
Blog: Hallmarks of Cancer: Genome Instability and Mutation
To overcome this, researchers can also target mechanisms that drive BRCA-related cancer resistance or look at ways to target DNA repair pathways that do not involve PARP.7 Additionally, preclinical and clinical trials are evaluating the efficacy of using PARP inhibitors in combination with other classes of drugs.8 Combination therapy strategies combining PARP inhibitors with cell-cycle checkpoint inhibitors, CDK inhibitors, drugs targeting epigenetic and post-translational modifications, and DNA damage agents are currently in progress. Studies leveraging immunotherapies are also of interest, as PARP inhibitors are being evaluated in combination with immune checkpoint inhibitors, antibody-drug conjugates, and engineered tumor-infiltrating lymphocytes.
Identifying how the BRCA mutation significantly increases the chances of developing cancer enables people with this mutation to take preventative steps. However, many develop breast cancer before realizing they carry the mutation. PARP inhibitors are the only FDA-approved targeted therapy available but are unfortunately limited due to the high rate of acquired resistance. Developing additional cancer therapeutics that can work separately or in tandem with PARP inhibitors will give people who are carriers more options to choose from when striving to completely eradicate their cancer.
23-can-91951 breast-cancer-blog
Select References
- Breastcancer.org. Breast Cancer Facts and Statistics. Updated May 13, 2025. https://www.breastcancer.org/facts-statistics
- National Breast Cancer Foundation. Early Detection of Breast Cancer. Updated April 16, 2025. https://www.nationalbreastcancer.org/early-detection-of-breast-cancer/
- Basser Center for BRCA. BRCA in men. https://www.basser.org/brca/brca-men.
- Roy R, Chun J, Powell SN. BRCA1 and BRCA2: different roles in a common pathway of genome protection. Nat Rev Cancer. 2011;12(1):67-68. Published 2011 Dec 23. doi:10.1038/nrc3181.
- Dilmac S, Ozpolat B. Mechanisms of PARP-Inhibitor-Resistance in BRCA-Mutated Breast Cancer and New Therapeutic Approaches. Cancers (Basel). 2023;15(14):3642. Published 2023 Jul 16. doi:10.3390/cancers15143642.
- Shah JB, Pueschl D, Wubbenhorst B, et al. Analysis of matched primary and recurrent BRCA1/2 mutation-associated tumors identifies recurrence-specific drivers. Nat Commun. 2022;13(1):6728. Published 2022 Nov 7. doi:10.1038/s41467-022-34523-y.
- Giudice E, Gentile M, Salutari V, et al. PARP Inhibitors Resistance: Mechanisms and Perspectives. Cancers (Basel). 2022;14(6):1420. Published 2022 Mar 10. doi:10.3390/cancers14061420.
- Luo L, Keyomarsi K. PARP inhibitors as single agents and in combination therapy: the most promising treatment strategies in clinical trials for BRCA-mutant ovarian and triple-negative breast cancers. Expert Opin Investig Drugs. 2022;31(6):607-631. doi:10.1080/13543784.2022.2067527.
23-CAN-91951
23-CAN-85595
G06